Duration of SARS-CoV-2 mRNA vaccine persistence and factors associated with cardiac involvement in recently vaccinated patients
Detection of BNT162b2 and mRNA-1273 vaccines in human tissues
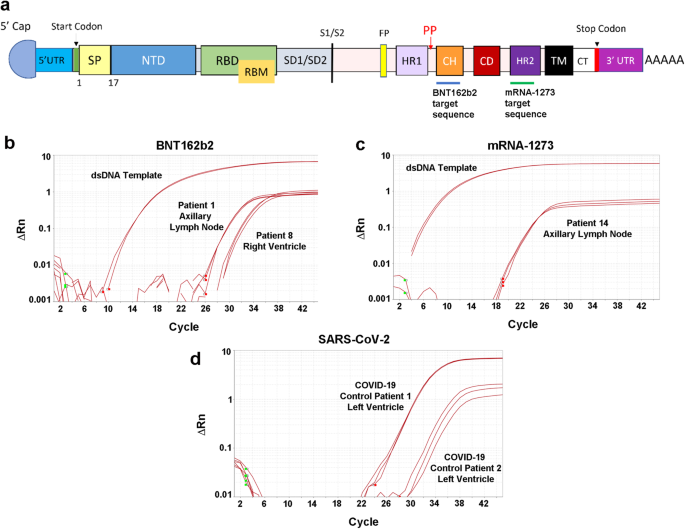
In the bilateral axillary lymph node samples, vaccine was detected in 2 (33%) of the 6 available samples from patients vaccinated with mRNA-1273 and in 6 (46%) of the 13 patients vaccinated with BNT162b2 (Figs. 1b, c, 2). Overall, for both vaccines, vaccine was detected in 8 (73%) of the 11 available axillary lymph nodes samples from the 12 patients dying within 30 days of vaccination compared with no detection of vaccine in any of the axillary lymph nodes samples from the 8 patients dying after 30 days from vaccination (P = 0.003, Fisher exact test). For none of the patients was vaccine detected in the liver, spleen, or mediastinal lymph nodes (each n = 19). For the 20 cardiac left ventricle and 20 cardiac right ventricle samples, vaccine was detected in 2 samples of left ventricle and 2 samples of right ventricle from a total of three patients. All three of these patients had been vaccinated with BNT162b2 within 30 days of death. All samples positive for vaccine were validated for sequences outside of the dsDNA control sequence (Supplementary Tables 3–4). Since SARS-CoV-2 can involve tissues throughout the body including the heart in the setting of severe respiratory tract infection22,23, as a further control, all tissue samples with detectable vaccine mRNA were screened for the SARS-CoV-2 virus E gene (Fig. 1d) and were found to be negative for the virus. Vaccine was not detected by RT-qPCR in any of the tissues from the 5 non-vaccinated control patients. Immunohistochemistry for the spike protein in the axillary lymph nodes, left ventricle, right ventricle and liver performed on all 20 vaccinated patients showed only non-specific staining (not shown).
Nachweis von BNT162b2- und mRNA-1273-Impfstoffen in menschlichen Geweben
In den bilateralen axillären Lymphknotenproben wurde der Impfstoff in 2 (33 %) der 6 verfügbaren Proben von mit mRNA-1273 geimpften Patienten und in 6 (46 %) der 13 mit BNT162b2 geimpften Patienten nachgewiesen (Abb. 1b, c, 2). Insgesamt wurde für beide Impfstoffe in 8 (73 %) der 11 verfügbaren axillären Lymphknotenproben der 12 Patienten, die innerhalb von 30 Tagen nach der Impfung starben, Impfstoff nachgewiesen, während in keiner der axillären Lymphknotenproben der 8 Patienten, die 30 Tage nach der Impfung starben, Impfstoff nachgewiesen wurde (P = 0,003, exakter Test nach Fisher). Bei keinem der Patienten wurde Impfstoff in der Leber, der Milz oder den mediastinalen Lymphknoten nachgewiesen (jeweils n = 19). Bei den 20 Proben aus der linken Herzkammer und den 20 Proben aus der rechten Herzkammer wurde der Impfstoff in 2 Proben aus der linken Herzkammer und 2 Proben aus der rechten Herzkammer von insgesamt drei Patienten nachgewiesen. Alle drei Patienten waren innerhalb von 30 Tagen vor ihrem Tod mit BNT162b2 geimpft worden. Alle Proben, die positiv auf den Impfstoff reagierten, wurden auf Sequenzen außerhalb der dsDNA-Kontrollsequenz validiert (siehe ergänzende Tabellen 3-4). Da SARS-CoV-2 Gewebe im gesamten Körper befallen kann
einschließlich des Herzens bei schweren Atemwegsinfektionen22,23, wurden als weitere Kontrolle alle Gewebeproben mit nachweisbarer Impfstoff-mRNA auf das E-Gen des SARS-CoV-2-Virus untersucht (Abb. 1d) und als negativ für das Virus befunden. In keinem der Gewebe der 5 nicht geimpften Kontrollpatienten wurde der Impfstoff mittels RT-qPCR nachgewiesen. Die immunhistochemische Untersuchung aller 20 geimpften Patienten auf das Spike-Protein in den axillären Lymphknoten, dem linken Ventrikel, dem rechten Ventrikel und der Leber ergab nur eine unspezifische Färbung (nicht gezeigt).
Übersetzt mit http://www.DeepL.com/Translator (kostenlose Version)
gut zu wissen wäre dann noch mit welchen chargen wurde geimpft... wenn ich an die dänische studie denke die mich bei manchen chargen an "nacl" denken lässt...
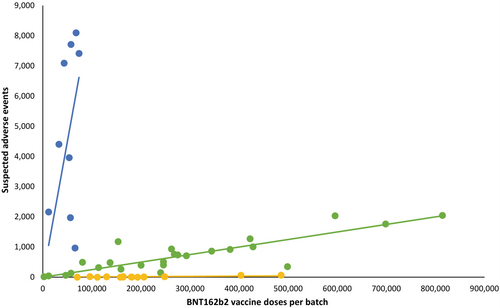
Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine
https://onlinelibrary.wiley.com/doi/10.1111/eci.13998